

Your calendar is perhaps the least reliable tool for determining when you are ready to play again. While many athletes circle a date six or nine months post-op, the biological reality of ligament maturation and neuromuscular control does not follow a standard clock. Achieving a safe return to sport after ACL surgery requires a shift from counting days to hitting specific, measurable performance markers. Research indicates that approximately 85 to 95 percent of individuals eventually return to their pre-injury activity levels, but the path there is often clouded by a fear of graft failure or the risk of tearing the opposite ACL.
It is natural to feel frustrated by a perceived lack of progress or to worry that your knee is not ready despite what the timeline suggests. You deserve a recovery plan that replaces guesswork with clinical data and professional certainty. This guide will help you master the objective milestones and functional phases required to safely return to competitive athletics after ACL reconstruction or repair. We will examine the five essential phases of recovery and the objective criteria, such as achieving at least 90 percent limb symmetry, that your surgical and rehab team uses to ensure your knee is truly prepared for the demands of the game.
Key Takeaways
- Learn why biological milestones and objective performance data are more critical for safety than a simple calendar timeline.
- Understand the essential early goals of recovery, including restoring full knee extension and normalizing your gait within the first few weeks.
- Discover the functional criteria and “hop test” batteries required to begin a jogging program and progress toward a full return to sport after ACL surgery.
- Identify strategies to manage kinesiophobia and use the ACL-RSI scale to ensure your psychological readiness matches your physical strength.
- Gain clarity on the final “Go/No-Go” criteria used by specialists to determine when you can safely return to high-impact contact sports.
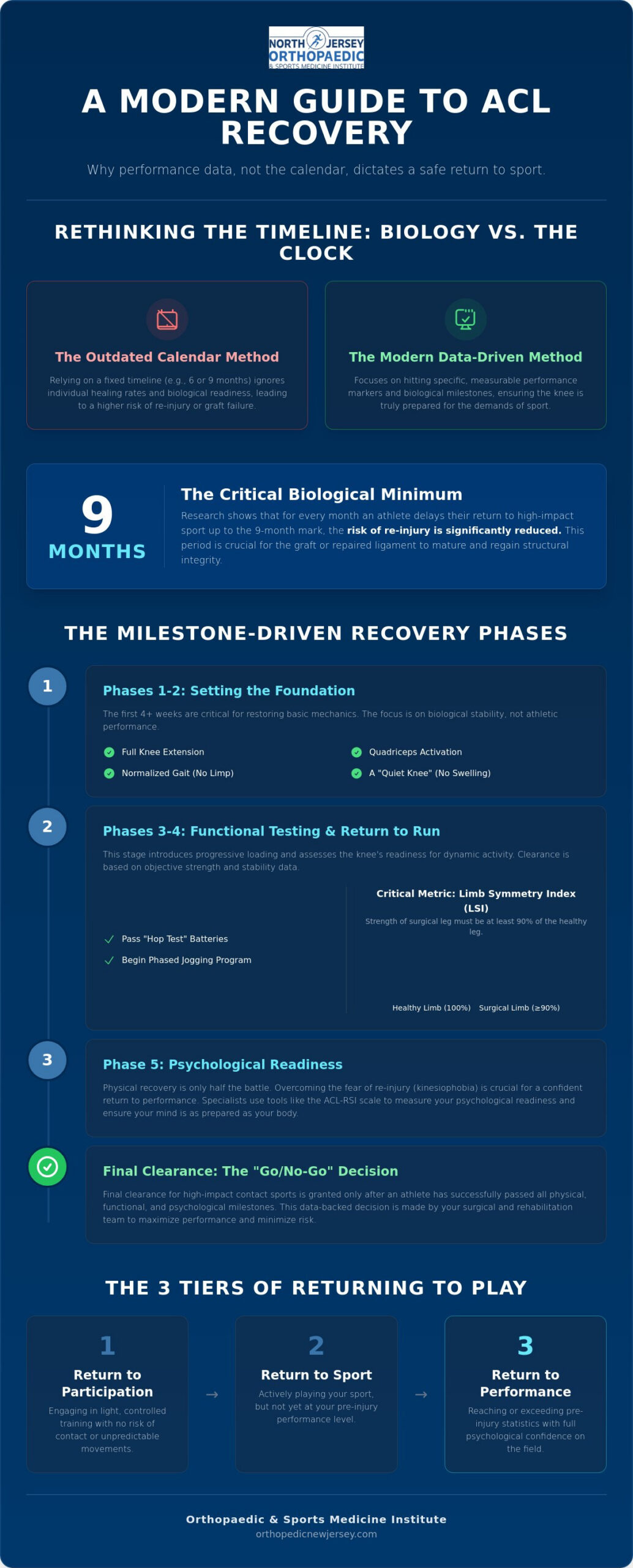
Understanding the ACL Recovery Timeline: Biology vs. The Calendar
Recovery is often misunderstood as a race against the clock. In reality, a successful return to sport after ACL surgery is a biological meritocracy. It relies on the cellular maturation of the tissue and the restoration of complex neuromuscular pathways. Rather than viewing clearance as a single date on a calendar, specialists view it as a multi-stage continuum where each phase must be earned through physical performance and physiological readiness.
For those undergoing traditional Anterior cruciate ligament reconstruction, the body must transform a tendon graft into a functional ligament. This process, known as ligamentization, involves three distinct phases: necrosis, revascularization, and remodeling. During the early months, the graft actually weakens as the body breaks down the original tendon cells before replacing them with new ligamentous tissue. This biological vulnerability is why returning too early often leads to graft failure.
Modern advancements have introduced sophisticated alternatives to traditional grafting. The BEAR implant ACL repair New Jersey athletes utilize represents a shift toward restorative medicine. Instead of replacing the ACL with a different tendon, this technology uses a bovine collagen implant to bridge the gap between torn ends. This encourages the body to heal its native ligament, preserving the original attachment points and mechanoreceptors that are often lost in standard reconstruction. This biological approach may offer different healing characteristics that your surgical team will monitor closely.
Regardless of the surgical technique, the nine month mark remains a critical biological minimum for most high impact sports. Research consistently shows that for every month return to sport after ACL surgery is delayed up to nine months, the risk of re injury is significantly reduced. This period allows the graft or repaired ligament to reach a level of structural integrity capable of withstanding the high torque of pivoting and jumping.
The 3 Stages of Returning to Play
Specialists categorize the final stages of rehab into three distinct tiers. Return to participation involves light, controlled training where there is no risk of contact or unpredictable movement. Return to sport occurs when the athlete participates in their specific discipline but remains below their previous performance levels. Finally, return to performance is achieved only when the athlete reaches or exceeds their pre injury statistics and regains full psychological confidence on the field.
Why Time-Based Clearance is Outdated
Relying solely on the calendar is a dangerous clinical practice. Every patient in Nutley and the surrounding communities heals at a different rate based on age, genetics, and adherence to physical therapy. A “quiet knee” is a non negotiable prerequisite for any progression. This means the joint is entirely free of effusion, which is medical swelling, and exhibits full range of motion. If an athlete returns to impact while the knee is still reactive, they risk chronic inflammation and long term joint degradation.
Phase 1 & 2: Setting the Foundation for Athletic Performance
The first four weeks following your procedure are the most critical for long-term success. While the final goal is a safe return to sport after ACL surgery, the immediate objective is biological stability and the restoration of basic mechanical function. You must prioritize two specific goals: achieving full, symmetrical knee extension and re-establishing quadriceps activation. Failing to regain the ability to fully straighten the knee early on can lead to permanent changes in joint mechanics and persistent gait abnormalities.
Before you can consider running or jumping, you must walk perfectly. Gait normalization, which means walking without a visible limp, is a non-negotiable prerequisite for advancing through rehab. This phase introduces the concept of progressive loading. By gradually increasing the mechanical stress placed on the healing tissue, we prepare the tendons and the graft for the future demands of explosive athletics. Working with a sports injury specialist Rutherford NJ athletes rely on ensures these early milestones are met with clinical precision, preventing the compensatory patterns that often lead to secondary injuries.
The Quadriceps Gold Standard
Quadriceps strength is the primary predictor of a successful return to play. We utilize the Limb Symmetry Index (LSI) to measure progress, with a 90 percent symmetry score serving as the benchmark for runners. You can monitor your progress at home through specific functional tests. Can you perform a straight leg raise without a “lag,” where the knee remains perfectly straight as the leg lifts? Can you achieve terminal knee extension while standing? These markers indicate that the muscle inhibition caused by surgery is resolving. Utilizing minimally invasive orthopedic surgery NJ techniques is often beneficial here, as smaller incisions and less tissue disruption typically lead to faster muscle reactivation.
Neuromuscular Control and Balance
Physical strength is only half of the equation. You must also re-establish the communication between your brain and your knee, a process known as proprioception. This involves specific drills that challenge your single-leg balance and spatial awareness. You must demonstrate stable, controlled balance on the operative leg before advancing to any “Return to Run” program. Furthermore, your training must incorporate core and hip stability. A strong posterior chain acts as a secondary stabilizer for the joint, protecting the new ACL from excessive rotational forces during future pivots and lateral movements.
If you find that your progress has plateaued or you are struggling to regain full range of motion, consulting a board-certified orthopedic specialist can help refine your protocol and keep your recovery on schedule.
Phase 3 & 4: Functional Testing and the ‘Return to Run’ Protocol
Progressing into the mid-to-late stages of recovery represents a transition from general strength to sport-specific function. Once the foundations of range of motion and initial quadriceps activation are secure, the focus shifts toward impact loading and explosive movement. A successful return to sport after ACL surgery requires a structured “Return to Run” protocol, typically initiated between 12 and 16 weeks post-op. This is not a fixed date; rather, it is a privilege earned once you demonstrate at least 80 percent quadriceps symmetry and a complete absence of pain or swelling during weight-bearing activities.
Managing your training load during this period is essential to avoid overuse injuries, such as patellar tendinopathy. We utilize a “step-wise” progression, starting with a walk-jog interval program on flat, predictable surfaces. The goal is to gradually expose the healing graft to the repetitive forces of running without triggering an inflammatory response. If the joint reacts with swelling or stiffness the following morning, the training load must be adjusted. This methodical approach ensures that the biological integrity of the joint is never compromised for the sake of speed.
The 5-Step Hop Test Battery
Functional testing is the most reliable way to measure your readiness for higher intensity. The hop test battery is a gold-standard assessment that compares the power and stability of your operative leg against your healthy limb. We look for a Limb Symmetry Index (LSI) of at least 90 percent across the following metrics:
- Single hop for distance: This measures raw power and your psychological confidence in landing on the repaired knee.
- Triple hop and crossover hop: These tests assess dynamic stability and your ability to control deceleration through multiple planes of motion.
- Timed 6-meter hop: This evaluates the combination of speed, power, and neuromuscular control over a set distance.
Agility and Reactive Training
True athletic performance is rarely predictable. While early agility drills involve planned movements around cones, the later stages of rehab must incorporate reactive training. This introduces a neurocognitive dimension where you must respond to external stimuli, such as a coach’s whistle or a partner’s movement. This “open-loop” training helps your brain “forget” the injury, reducing the hesitation that often leads to re-injury during a game. Utilizing the advanced diagnostic tools at a sports medicine clinic Montclair NJ athletes trust allows for precise tracking of these reactive patterns, ensuring you are physically and mentally prepared for the chaos of competitive play.
As you move through these functional phases, the objective data gathered from these tests provides the confidence needed to transition from the clinic back to the field. This evidence-based progression is the safest way to navigate the final steps of your return to sport after ACL surgery.
Psychological Readiness: Overcoming the Fear of Re-injury
Physical strength is only one component of a successful return. Many athletes pass their hop tests and strength assessments but remain hesitant once they step back onto the field. This mental gap is often the primary reason why even elite competitors fail to return to their pre-injury level of performance. A safe return to sport after ACL surgery requires your brain to trust your knee as much as your surgeon does.
To quantify this readiness, specialists utilize the ACL-RSI (Anterior Cruciate Ligament, Return to Sport after Injury) scale. This validated tool measures your emotions, confidence in your performance, and risk appraisal. If your score is low, you’re statistically at a higher risk for a secondary ACL tear, regardless of how strong your quadriceps have become. High physical performance without psychological readiness creates a dangerous disconnect during the split-second decisions required in competitive play.
The Link Between Confidence and Biomechanics
Hesitation isn’t just a feeling; it fundamentally changes how you move. When an athlete is fearful, they often adopt a “stiff-legged” landing pattern or avoid shifting weight onto the operative limb. These protective mechanisms are counterproductive, as they increase the impact forces on the joint and place the new graft at greater risk. Kinesiophobia is defined as an irrational and debilitating fear of physical movement resulting from a feeling of vulnerability to painful injury or re-injury.
You can combat this through gradual exposure and mental conditioning. Visualization and mental imagery during the middle months of rehab keep the neural pathways for athletic movement active. Gradually reintroducing sport-specific environments, such as standing on the sidelines or participating in non-contact drills, helps desensitize the brain to the “threat” of the field. This process allows you to rebuild on-field confidence in a controlled, step-wise fashion.
Building a Support System in North Jersey
You shouldn’t have to guess when you’re ready to play again. A board certified orthopedic surgeon NJ provides the clinical anchor for your recovery. This specialist coordinates with your physical therapist and coaches to ensure that every member of your team is looking at the same objective data before giving the final “green light.” This unified approach reduces the anxiety of the “unknown” and provides a clear roadmap for your return.
Don’t ignore the social isolation that often accompanies a long-term injury. Being away from the team can be as taxing as the physical rehab itself. Staying involved in team meetings, video sessions, or even helping with equipment can maintain your identity as an athlete. This social connection is vital as you navigate the final stages of your return to sport after ACL surgery.
If you’re feeling a lack of confidence in your knee’s stability, contact a board-certified specialist to perform a comprehensive functional and psychological assessment.
Final Clearance: Navigating the Return to High-Impact Sport
The final clearance for contact sports like football, soccer, and lacrosse is a complex clinical determination. It is the culmination of months of disciplined work, and the “Go/No-Go” decision involves a synthesis of all previous milestones. You must demonstrate a quiet knee, 90 percent limb symmetry in strength and hop testing, and a high ACL-RSI score. This phase culminates in a formal “Return to Play” meeting. During this session, the surgeon, athlete, and parents review the objective data to ensure everyone understands the remaining risks and the necessity of a gradual reintegration into full-speed play.
Consulting a sports injury doctor Kearny NJ athletes trust provides an opportunity for a final, rigorous assessment or a second opinion before returning to the field. This ensures that your return to sport after ACL surgery is supported by the highest standards of orthopedic care and that no functional deficits remain. This professional oversight is the bridge between a successful rehab and a safe return to competitive athletics.
Sport-Specific Considerations for NJ Athletes
Playing surfaces in North Jersey high schools significantly impact joint stress. Many local programs utilize artificial turf, which provides higher friction than natural grass. This increased “grip” can lead to higher rotational torque on the knee during sudden pivots. Athletes must practice their cutting and deceleration drills on the specific surfaces they’ll encounter during the season to ensure their mechanics remain sound under these high-torque conditions.
Seasonal timing often presents the greatest psychological challenge. We frequently see athletes attempt to rush their rehab to participate in “Senior Night” or playoff rounds. However, the biological integrity of the graft doesn’t accelerate for a schedule. Returning prematurely for a single game can jeopardize your long-term joint health and increase the risk of a secondary tear. Regarding bracing, while a post-operative functional brace can provide a sense of security and protect against external lateral impacts during the first season back, it’s not a substitute for the neuromuscular control developed during physical therapy.
The Road Ahead: Prevention as a Lifestyle
Your discharge from formal therapy isn’t the end of your journey. To prevent a contralateral ACL tear, which occurs in approximately 5 to 10 percent of athletes within five years of the initial surgery, prevention must become a lifestyle. Integrating evidence-based programs like the FIFA 11+ or the PEP program into your daily warm-ups reduces re-injury risk by 50 to 70 percent in certain sports. These programs focus on landing mechanics and eccentric strength, which are vital for long-term joint preservation.
Annual “tune-ups” with your orthopedic specialist are recommended to monitor strength symmetry and joint stability. Modern ACL procedures in Nutley and the surrounding communities have high success rates, with 85 to 95 percent of patients returning to their pre-injury activities. By prioritizing objective milestones over the calendar, you can rejoin your team with the confidence that your knee is structurally and functionally prepared for the demands of competition. Your return to sport after ACL surgery is a major milestone, and maintaining these habits will ensure you stay on the field for years to come.
Securing Your Athletic Future
Transitioning from the clinic to the competitive arena is a process defined by objective data and biological readiness. By prioritizing quadriceps symmetry and passing rigorous functional hop tests, you move beyond the limitations of a traditional calendar-based approach. Addressing psychological barriers is equally vital, ensuring your mental confidence matches your physical restoration. A safe return to sport after ACL surgery is achievable when you adhere to a milestone-based protocol that respects the biology of healing.
As a board-certified orthopedic surgeon specializing in advanced techniques like the BEAR® Implant, our team provides the specialized expertise necessary for athletes in Nutley, Montclair, and across North Jersey. We invite you to Schedule an ACL Recovery Consultation in Nutley Today to receive a comprehensive evaluation of your current progress and functional readiness. Your dedication to a structured, evidence-based recovery is the foundation for a resilient and high-performing future on the field. We’re here to guide you through every milestone of your journey back to the game.
Frequently Asked Questions
What is the fastest I can return to sports after ACL surgery?
The average timeframe for a safe return to sport after ACL surgery is 9 to 12 months for traditional reconstructions. While some primary repairs may allow for a return in approximately 6 months, these are reserved for specific tear types and carry different risks. Rushing the process increases the likelihood of graft failure; biological maturation of the tissue simply cannot be forced by a calendar date.
Is it normal to have knee clicking or popping when returning to sport?
Auditory sensations like clicking or popping are common and often result from scar tissue or minor joint surface changes. If these sounds occur without associated pain, instability, or new swelling, they’re generally considered benign. However, if a “pop” is accompanied by immediate effusion or a feeling of the knee giving way, you should contact your surgeon for a clinical evaluation.
Do I need a knee brace to play sports after an ACL reconstruction?
A functional brace is not a clinical requirement for most athletes once they’ve achieved full strength and neuromuscular control. Many specialists recommend a brace during the first season back for psychological reassurance and protection against external lateral impacts in contact sports. It’s vital to remember that a brace cannot compensate for deficits in quadriceps strength or poor landing mechanics.
What are the signs that I am progressing too quickly in my rehab?
The primary indicator of overexertion is joint effusion, or swelling, that appears after a training session or the following morning. Persistent pain that lasts more than 24 hours or a sudden loss of terminal knee extension also suggests the joint is not yet ready for the current training load. If the knee becomes reactive, it’s a signal to reduce intensity until the inflammation subsides.
Why is the risk of tearing the other ACL so high after surgery?
Research indicates a 5 to 10 percent risk of tearing the contralateral ACL within five years of the initial injury. This high rate is often due to continued biomechanical compensations, where the athlete over-relies on the healthy leg. The same anatomical or genetic factors that contributed to the first tear remain present, making ongoing neuromuscular training essential for protecting both knees.
Can the BEAR® implant speed up my return to sport compared to a traditional graft?
The BEAR® implant focuses on native ligament healing, which may offer a different recovery trajectory for eligible patients. Because it preserves the original attachment points and mechanoreceptors, some athletes report a more “natural” feel during early rehab. While it represents a modern alternative to reconstruction, the timeline for a full return to sport after ACL surgery still depends on meeting objective strength and stability milestones.
How do I know if my quadriceps are strong enough for running?
Clinical benchmarks require a Limb Symmetry Index (LSI) of at least 80 to 90 percent before you begin a jogging program. You can monitor this through functional markers like the ability to perform a straight leg raise without a lag and maintaining stable single-leg balance. A professional evaluation using a dynamometer provides the most accurate data to ensure your quadriceps can safely absorb running forces.
What happens if I fail my return-to-sport functional tests?
Failing a functional test is not a permanent setback; it’s a diagnostic tool that identifies specific weaknesses. If you don’t meet the 90 percent symmetry requirement, your team will adjust your program to target those deficits, whether they’re in explosive power, deceleration, or reactive control. Retesting typically occurs every 4 to 6 weeks until you demonstrate the stability required for safe competition. For athletes dealing with concurrent knee conditions, working with a meniscus tear specialist NJ athletes rely on can help address any additional structural issues that may be affecting your test results and overall recovery trajectory.


